Our objective was to know the bacteriological profile of nosocomial infections and determine the risk factors in order to effectively fight against this scourge. Descriptive and retrospective study carried out in our department from April 30 to December 31, 2023, i.e. a period of 8 months. A total of 105 patients operated on for clean surgery were enrolled with a sex ratio of 9.5 ∕1 in favour of male sex. They came from the Sikasso region and the neighbouring countries (RCI and B Faso). Average age: 54.77±21.70 (3-85 years). Antibiotic prophylaxis based on ceftriaxone or Amoxy Clavulanic Acid instituted in all our patients. 15/105 developed a nosocomial infection, i.e. an incidence of 14.28%. The two types of infection are: Surgical site infection SSI, which is the predominant form with a rate of 73.30%, followed by infection associated with urethral catheterization, i.e. 26.66%. Cytobacteriological analysis of the samples made it possible to isolate germs in 13 patients, while they were sterile in the other two. These E Coli and K Pneumonia germs have been shown to be sensitive to imipenem, amikacin and fosfomycin. Length of stay, history of bladder catheterization and classic open surgery were proven risk factors. Nosocomial infection remains a real public health problem. Fighting against this scourge requires the establishment of regular monitoring system and good prevention policy based on strengthening hygiene and aseptic measures, promoting rational prescribing and combating self-medication.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Nosocomial infection NI or acquired healthcare-associated infection is an infection contracted by a patient during 48 hours after admission in health facility.
According to WHO
[1]
Vela Navarrete R, Soriano F et al. Urinary tract Infections caused by permanent catheterization: Natural history, mechanisms and prevention strategies. Arch Esp Urol. 2007; 60: 49-56.
[2]
WHO, prevention of hospital acquired infection. A practical guide 2eme edition 2013.
[1, 2]
the incidence of NI is becoming increasingly high worldwide. The reasons for this increase differ according to health care system development. In the West, the high frequency of aggressive gestures in neonatal units, surgical departments and intensive care, especially on patients with a certain comorbidity related to extreme age, provide an environment conducive to the selection, proliferation and transmission of multi-resistant germs such as MRSA (methicillin-resistant staphylococcus aureus), VRE (vancomycin resistant enterococcus), ESBLs (Extended spectrum beta lactamases excreted enter bacteria)
[3]
Ewans TM, Ortiz CR and LaForce FM (1999) Prevention and Control of Nosocomial Infection in the Intensive Care Unit. Intensive Care Medi.
[4]
Vincent JL, Marshall J, Silva E, Anzueto A, Martin CD, Moreno R, et al. International study of the prevalence and outcomes of infection in intensive care units. JAMA 2009; 30.
[3, 4]
. On the other hand, in our African context, it must be recognized that this scourge could be the result of non-compliance with aseptic and hygienic rules, the irrational use of antibiotics in our structures; self-medication, illicit sale of medicines and misuse of antibiotics in agro pastoral and fish farming activities. In view of the increase in the length of hospitalization with its corollary of additional costs, the increase in the morbidity and mortality rate that they cause. Today those infections became a real public health problem and a major challenge for us hospital practitioners as well as for biologists and health authorities
[5]
Klevens RM, Edwards JR, Richards CL, et al. (2007) Estimating health care-associated infections and deaths in U.S. hospitals, 2002. Public Health Rep 122: 160–166. Lambert ML, Suetens C, Savey A.
[5]
.
The aims of this study was to:
Study the bacteriological profile of nosocomial infections; determining their risk factors and facilitate implementation of measures for prevention.
2. Materials and Methods
2.1. Study Design
This was a descriptive and retrospective study carried out in the urology department of the Sikasso hospital from April 30, 2023 to December 31, 2023, i.e. a period of 8 months.
2.2. Study Population and Sampling
Population: All patients who were hospitalized for at least 48 hours in our department and who had no obvious infection on admission.
Inclusion: All patients who have shown infection signs during hospitalisation and this 2-30 days after admission.
Non-inclusion: those who have not reached 48 hours in the service have not been included.
Exclusion: Patients treated for community-acquired infectious diseases (urinary, cutaneous or systemic infection) and cases of fistula managed during the campaign of MCS / USAID are excluded from this study.
2.3. Data Collection and Analysis
Hospitalization records and operative report registers were used for data collection Information about epidemiological, socio-demographic aspects; Clinical and biological signs as well as therapeutic management were collected.
Data analysis was performed by IBM-SPSS20 software.
Multivariate logistic regression or Fisher’s exact test were used to evaluate correlations.
3. Results
We collected a total of 105 patients, 95 of whom were male and 10 female; sex ratio 9.5 ∕1 in favour of male sex. Patients were from Sikasso region and border countries (Republic of Côte d'Ivoire and Burkina Faso) respectively 82.15%, 13.20% and 5.10%.
Mean age was 54.77±21.70 (3-85 years)
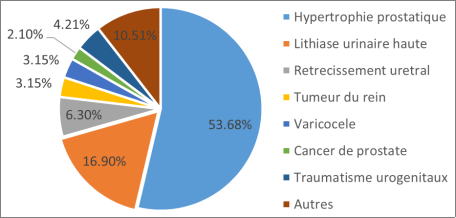
A total of 105 patients were treated in our department, the majority of whom (95%) had 1-2 as ASA score and it was generally a scheduled surgery (94.70%).
All of them benefited from antibiotic prophylaxis based on either ceftriaxone or Amoxy Clavulanic Acid, administered just before anaesthetic induction. Out of them, 15 patients developed a nosocomial infection, an incidence of 14.28%. Mean time of NI onset is 8.10 days (4-22 days). The two types of hospital-acquired nosocomial infection recorded are:
SSI surgical site infection is the predominant form (11/15) or 73.30% of cases of infection, followed by urethral catheterization-associated infection CAUTI (26.66%).
The different clinical manifestations associated with infections are: Suppuration of the surgical wound with discharge of purulent or serohematic fluid and loosening of the threads; acute scrotal pain and swelling accompanied by fever, cloudy urine and burning urination.
Cytobacteriological analysis of the sample taken from surgical wound and urine isolated germs in 13 patients, while they were sterile in the other two. The germs isolated from different samples were mainly multidrug-resistant bacteria consisting of: Escherichia coli, Klebsiella Pneumonia and Staphylococcus aureus. They showed strong resistance to Amoxicillin-clavulanic acid, ceftriaxone and ciprofloxacin.
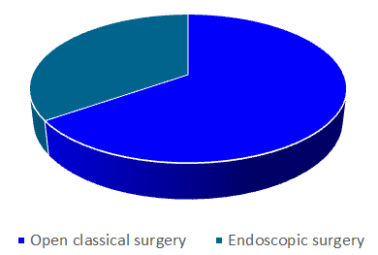
No clear correlation was found between sex, age and the occurrence of nosocomial infections. However, significant correlation exists between the length of stay, bladder catheterization history, open classic surgery and nosocomial infection occurrence, respectively.
OR: 2. P = 0.000 (95% CI=1.279-2.048); OR: 9.75 P = 0.018 (95% CI=1.473-0.083);
Figure 3. Profile of germs sensibility and resistance to antibiotics.
Table 1. Distribution according isolated germs responsible of NI.
Isolated Germs /CBEP + CBEU
Number
Percentage
BGN Bacillus gram negative
12
80.00%
Escherichia Coli
06
Klebsiela Pneumonia
05
E Coli+ K Pneumonia
01
CGP Cocci gram positif
01
6,66%
Staphylococcus Aureus
01
Sterile Sample
02
13.66%
Total
15
100%
4. Discussion
Our prevalence of nosocomial infections is quite high compared to that reported by O K Ige et al
[6]
Ok ige, AA Adesenmi, MC Asuzu et al. Hospital acquired infection in Nigerian tertiary health facility: an audit of surveillance reports. Niger Med J. 2011 Oct-Dec; 52(4): 239–243.
[6]
. While it is almost similar to that of E Dridi et al
[7]
E dridi, A chetoul, A Zaoui et al. Prevalence de l’infection nosocomiale dans un hospital regional tunisien. Santé publique 2006; 182: 187-94.
[7]
. The first is a cross-sectional study carried out in a 3rd reference hospital. Whereas ours was carried out in a department of the surgical specialties of a 2nd reference hospital which, moreover, lacks a rigorous surveillance system focused on the search for and identification of germs in risk areas, and a program for the prevention and control of nosocomial infection. As reported by previous studies
[8]
Bajaddoub Z, Moudouni S. M. Facteurs de risque des infections urinaires nosocomiales: étude prospective randomisée. Thèse Doctorat Médecine; Marrakech 2008, N°97, 91p.
[9]
Apanga S, Adda J, Issahaku M, Amofa J, et al. Post-operative surgical site infection in a surgical ward of a tertiary care hospital in Northern Ghana. Int. J. Res. Health Sci. 2014; 2: 207-21.
[8, 9]
, the predominant types of nosocomial infections in our department are SSI surgical site infections and urinary tract infections. They both gave rise to suggestive clinical features:
These are respectively a fever ≥38 C, a purulent discharge, the loosening of the threads and wound dehiscence often followed by a vesico-cutaneous fistula. A fever ≥38C accompanied by scrotal pain and swelling associated with urination burning, cloudy appearance of the urine or pyuria. Biologically, the presence of polynuclear hyperleukocytosis and leukocyturia Bacteriological examinations of samples taken from the wounds and urine of patients with these complications have identified and isolated mainly gram-negative bacteria, including Escherichia Coli and Klebsiella Pneumonia.
This high prevalence of nosocomial infections both in our series and in other African studies
[10]
Kallel H, Bahloul M, Ksibi H et al. Prevalence of hospital-acquired Infection in a Tunisian hospital. J Hosp Infect 2005; 59(4): 343-7.
[10]
denotes inadequacies in the implementation of measures to combat and prevent nosocomial infections within our health structures in terms of compliance with the rules and principles of good hygiene, rigor in the sterilization of equipment and aseptic rules in the execution of pre- and post-operative care.
The majority of our patients had a very good general condition illustrated by the fact that 90% of them belonged to ASA 1-2 group. In addition, no correlation was found between sex, age and the occurrence of a nosocomial infection. The only proven risk factors for the occurrence of this type of infection remain the length of hospitalization, procedures such as bladder catheterization and the open nature of the surgery. This sufficiently proves the existence of flaws in the processes of disinfection and sterilization of equipment and premises; the lack of respect for hygiene and aseptic rules during the performance of care both in the operating room and in our inpatient departments.
Gram-negative bacilli like Escherichia Coli and Klebsiela Pneumonia are the germs responsible for nosocomial infections in our series. Their antibiotic resistance profile is consistent with the literature
[11]
Azeez-Akande O. Emerging and reemerging infectious agents of nosocomial diseases – The need for review of hospital policy and control strategies. Bayero J. Pure App. Sci. 2012; 5: 19–25.
[12]
Patil A, Patil K, Pankaj Pawar P et al. Isolation and survey of antibiotic sensitivity in nosocomial infections in North Maharashtra Region. Journal of Physician's Association of India. 2013; 61: 454-58.
[11, 12]
. There is a strong resistance to the action of amoxicillin-clavulanic acid and ceftriaxone, which are our preferred molecules in antibiotic prophylaxis. Hence the need to use antibiotics in prophylaxis that have less impact on our environment. Nevertheless, those germs have been shown to be sensitive to the action of antibiotics such as imipenem, amikacin and fosfomycin...
The consequences of NI depend on its nature and can be serious, even compromising the functional, aesthetic or even vital prognosis. Unlike other series
[13]
Vital signs: Central line–associated blood stream infections – United States, 2001, 2008, and 2009. Morb Mortal Wkly Rep 2011; 60(08): 243-8.
[13]
both our studies and others
[14]
Samuel SO, Kayode OO, Musa OI, et al. Nosocomial infections and the challenges of control in developing Countries. Afr. J. Clin. Exp. Microbiol. 2010; 11: 102-110.
[15]
Tohme A, Karam-Sarkis D, El-rassi R et al. Agents and consequences of nosocomial Infections in a Lebanese University Retrospective study over a 2 year period. Ann Med Interne 2001; 152(2): 77-83.
[14, 15]
where SSI and C-AUTI were predominant, no deaths have been recorded. But despite everything, these complications, with its corollary of increased treatment time, multiplication of means for investigation and overconsumption of drugs, especially the latest generation of antibiotics, contribute in serious psychological and socio-economic consequences.
5. Conclusion
The implementation of a good policy to promote rational prescribing; Fighting against self-medication, the illicit sale of medicines as well as compliance with regulatory standards for the use of antibiotics in agro pastoral and poultry activities are necessary in order to reduce the emergence of multi-resistant strains.
Fighting against this scourge requires the establishment of a regular and rigorous surveillance system in order to detect multi-resistant germs, use physicochemical means and appropriate measures to stop their transmission.
Limiting hospital stays, compliance with aseptic and hygienic rules and proper management of our biomedical waste could also be crucial to control this scourge of nosocomial infection.
Abbreviations
NI
Nosocomial Infection
ASA
American Society of Anaesthesiologists
SSI
Surgical Site Infection
CBEU
Cytobacteriological Examination of Urine
CBEP
Cytobacteriological Examination of Pus
CAUTI
Catheter Associated Urinary Tract Infection
WHO
World Health Organisation
MCS / USAID
Momentum Safe Surgery / United States Agency for International Development
Conflicts of Interest
The authors declare no conflicts of interest.
References
[1]
Vela Navarrete R, Soriano F et al. Urinary tract Infections caused by permanent catheterization: Natural history, mechanisms and prevention strategies. Arch Esp Urol. 2007; 60: 49-56.
[2]
WHO, prevention of hospital acquired infection. A practical guide 2eme edition 2013.
[3]
Ewans TM, Ortiz CR and LaForce FM (1999) Prevention and Control of Nosocomial Infection in the Intensive Care Unit. Intensive Care Medi.
[4]
Vincent JL, Marshall J, Silva E, Anzueto A, Martin CD, Moreno R, et al. International study of the prevalence and outcomes of infection in intensive care units. JAMA 2009; 30.
[5]
Klevens RM, Edwards JR, Richards CL, et al. (2007) Estimating health care-associated infections and deaths in U.S. hospitals, 2002. Public Health Rep 122: 160–166. Lambert ML, Suetens C, Savey A.
[6]
Ok ige, AA Adesenmi, MC Asuzu et al. Hospital acquired infection in Nigerian tertiary health facility: an audit of surveillance reports. Niger Med J. 2011 Oct-Dec; 52(4): 239–243.
[7]
E dridi, A chetoul, A Zaoui et al. Prevalence de l’infection nosocomiale dans un hospital regional tunisien. Santé publique 2006; 182: 187-94.
[8]
Bajaddoub Z, Moudouni S. M. Facteurs de risque des infections urinaires nosocomiales: étude prospective randomisée. Thèse Doctorat Médecine; Marrakech 2008, N°97, 91p.
[9]
Apanga S, Adda J, Issahaku M, Amofa J, et al. Post-operative surgical site infection in a surgical ward of a tertiary care hospital in Northern Ghana. Int. J. Res. Health Sci. 2014; 2: 207-21.
[10]
Kallel H, Bahloul M, Ksibi H et al. Prevalence of hospital-acquired Infection in a Tunisian hospital. J Hosp Infect 2005; 59(4): 343-7.
[11]
Azeez-Akande O. Emerging and reemerging infectious agents of nosocomial diseases – The need for review of hospital policy and control strategies. Bayero J. Pure App. Sci. 2012; 5: 19–25.
[12]
Patil A, Patil K, Pankaj Pawar P et al. Isolation and survey of antibiotic sensitivity in nosocomial infections in North Maharashtra Region. Journal of Physician's Association of India. 2013; 61: 454-58.
[13]
Vital signs: Central line–associated blood stream infections – United States, 2001, 2008, and 2009. Morb Mortal Wkly Rep 2011; 60(08): 243-8.
[14]
Samuel SO, Kayode OO, Musa OI, et al. Nosocomial infections and the challenges of control in developing Countries. Afr. J. Clin. Exp. Microbiol. 2010; 11: 102-110.
[15]
Tohme A, Karam-Sarkis D, El-rassi R et al. Agents and consequences of nosocomial Infections in a Lebanese University Retrospective study over a 2 year period. Ann Med Interne 2001; 152(2): 77-83.
Traoré, S., Dembélé, O., Traore, M., Ouattara, K. S., Berthé, O., et al. (2025). Bacteriological Profile, Prevention and Control of Nosocomial Infections. American Journal of Biomedical and Life Sciences, 13(1), 31-35. https://doi.org/10.11648/j.ajbls.20251301.15
Traoré, S.; Dembélé, O.; Traore, M.; Ouattara, K. S.; Berthé, O., et al. Bacteriological Profile, Prevention and Control of Nosocomial Infections. Am. J. Biomed. Life Sci.2025, 13(1), 31-35. doi: 10.11648/j.ajbls.20251301.15
Traoré S, Dembélé O, Traore M, Ouattara KS, Berthé O, et al. Bacteriological Profile, Prevention and Control of Nosocomial Infections. Am J Biomed Life Sci. 2025;13(1):31-35. doi: 10.11648/j.ajbls.20251301.15
@article{10.11648/j.ajbls.20251301.15,
author = {Salifou Traoré and Ousmane Dembélé and Madou Traore and Kateneme Seydou Ouattara and Oumar Berthé and Siaka Coulibaly and Aly Diallo and Bathio Traoré and Moussa Diassana and Bernard Coulibaly and Ahmadou Dembélé and Abdou Dolo and Moussa Kanté and Soumaila Traoré and Moussa Coulibaly and Ternan Traoré and Luka Diarra and Hassan Souleymane},
title = {Bacteriological Profile, Prevention and Control of Nosocomial Infections},
journal = {American Journal of Biomedical and Life Sciences},
volume = {13},
number = {1},
pages = {31-35},
doi = {10.11648/j.ajbls.20251301.15},
url = {https://doi.org/10.11648/j.ajbls.20251301.15},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajbls.20251301.15},
abstract = {Our objective was to know the bacteriological profile of nosocomial infections and determine the risk factors in order to effectively fight against this scourge. Descriptive and retrospective study carried out in our department from April 30 to December 31, 2023, i.e. a period of 8 months. A total of 105 patients operated on for clean surgery were enrolled with a sex ratio of 9.5 ∕1 in favour of male sex. They came from the Sikasso region and the neighbouring countries (RCI and B Faso). Average age: 54.77±21.70 (3-85 years). Antibiotic prophylaxis based on ceftriaxone or Amoxy Clavulanic Acid instituted in all our patients. 15/105 developed a nosocomial infection, i.e. an incidence of 14.28%. The two types of infection are: Surgical site infection SSI, which is the predominant form with a rate of 73.30%, followed by infection associated with urethral catheterization, i.e. 26.66%. Cytobacteriological analysis of the samples made it possible to isolate germs in 13 patients, while they were sterile in the other two. These E Coli and K Pneumonia germs have been shown to be sensitive to imipenem, amikacin and fosfomycin. Length of stay, history of bladder catheterization and classic open surgery were proven risk factors. Nosocomial infection remains a real public health problem. Fighting against this scourge requires the establishment of regular monitoring system and good prevention policy based on strengthening hygiene and aseptic measures, promoting rational prescribing and combating self-medication.},
year = {2025}
}
TY - JOUR
T1 - Bacteriological Profile, Prevention and Control of Nosocomial Infections
AU - Salifou Traoré
AU - Ousmane Dembélé
AU - Madou Traore
AU - Kateneme Seydou Ouattara
AU - Oumar Berthé
AU - Siaka Coulibaly
AU - Aly Diallo
AU - Bathio Traoré
AU - Moussa Diassana
AU - Bernard Coulibaly
AU - Ahmadou Dembélé
AU - Abdou Dolo
AU - Moussa Kanté
AU - Soumaila Traoré
AU - Moussa Coulibaly
AU - Ternan Traoré
AU - Luka Diarra
AU - Hassan Souleymane
Y1 - 2025/02/10
PY - 2025
N1 - https://doi.org/10.11648/j.ajbls.20251301.15
DO - 10.11648/j.ajbls.20251301.15
T2 - American Journal of Biomedical and Life Sciences
JF - American Journal of Biomedical and Life Sciences
JO - American Journal of Biomedical and Life Sciences
SP - 31
EP - 35
PB - Science Publishing Group
SN - 2330-880X
UR - https://doi.org/10.11648/j.ajbls.20251301.15
AB - Our objective was to know the bacteriological profile of nosocomial infections and determine the risk factors in order to effectively fight against this scourge. Descriptive and retrospective study carried out in our department from April 30 to December 31, 2023, i.e. a period of 8 months. A total of 105 patients operated on for clean surgery were enrolled with a sex ratio of 9.5 ∕1 in favour of male sex. They came from the Sikasso region and the neighbouring countries (RCI and B Faso). Average age: 54.77±21.70 (3-85 years). Antibiotic prophylaxis based on ceftriaxone or Amoxy Clavulanic Acid instituted in all our patients. 15/105 developed a nosocomial infection, i.e. an incidence of 14.28%. The two types of infection are: Surgical site infection SSI, which is the predominant form with a rate of 73.30%, followed by infection associated with urethral catheterization, i.e. 26.66%. Cytobacteriological analysis of the samples made it possible to isolate germs in 13 patients, while they were sterile in the other two. These E Coli and K Pneumonia germs have been shown to be sensitive to imipenem, amikacin and fosfomycin. Length of stay, history of bladder catheterization and classic open surgery were proven risk factors. Nosocomial infection remains a real public health problem. Fighting against this scourge requires the establishment of regular monitoring system and good prevention policy based on strengthening hygiene and aseptic measures, promoting rational prescribing and combating self-medication.
VL - 13
IS - 1
ER -
Traoré, S., Dembélé, O., Traore, M., Ouattara, K. S., Berthé, O., et al. (2025). Bacteriological Profile, Prevention and Control of Nosocomial Infections. American Journal of Biomedical and Life Sciences, 13(1), 31-35. https://doi.org/10.11648/j.ajbls.20251301.15
Traoré, S.; Dembélé, O.; Traore, M.; Ouattara, K. S.; Berthé, O., et al. Bacteriological Profile, Prevention and Control of Nosocomial Infections. Am. J. Biomed. Life Sci.2025, 13(1), 31-35. doi: 10.11648/j.ajbls.20251301.15
Traoré S, Dembélé O, Traore M, Ouattara KS, Berthé O, et al. Bacteriological Profile, Prevention and Control of Nosocomial Infections. Am J Biomed Life Sci. 2025;13(1):31-35. doi: 10.11648/j.ajbls.20251301.15
@article{10.11648/j.ajbls.20251301.15,
author = {Salifou Traoré and Ousmane Dembélé and Madou Traore and Kateneme Seydou Ouattara and Oumar Berthé and Siaka Coulibaly and Aly Diallo and Bathio Traoré and Moussa Diassana and Bernard Coulibaly and Ahmadou Dembélé and Abdou Dolo and Moussa Kanté and Soumaila Traoré and Moussa Coulibaly and Ternan Traoré and Luka Diarra and Hassan Souleymane},
title = {Bacteriological Profile, Prevention and Control of Nosocomial Infections},
journal = {American Journal of Biomedical and Life Sciences},
volume = {13},
number = {1},
pages = {31-35},
doi = {10.11648/j.ajbls.20251301.15},
url = {https://doi.org/10.11648/j.ajbls.20251301.15},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajbls.20251301.15},
abstract = {Our objective was to know the bacteriological profile of nosocomial infections and determine the risk factors in order to effectively fight against this scourge. Descriptive and retrospective study carried out in our department from April 30 to December 31, 2023, i.e. a period of 8 months. A total of 105 patients operated on for clean surgery were enrolled with a sex ratio of 9.5 ∕1 in favour of male sex. They came from the Sikasso region and the neighbouring countries (RCI and B Faso). Average age: 54.77±21.70 (3-85 years). Antibiotic prophylaxis based on ceftriaxone or Amoxy Clavulanic Acid instituted in all our patients. 15/105 developed a nosocomial infection, i.e. an incidence of 14.28%. The two types of infection are: Surgical site infection SSI, which is the predominant form with a rate of 73.30%, followed by infection associated with urethral catheterization, i.e. 26.66%. Cytobacteriological analysis of the samples made it possible to isolate germs in 13 patients, while they were sterile in the other two. These E Coli and K Pneumonia germs have been shown to be sensitive to imipenem, amikacin and fosfomycin. Length of stay, history of bladder catheterization and classic open surgery were proven risk factors. Nosocomial infection remains a real public health problem. Fighting against this scourge requires the establishment of regular monitoring system and good prevention policy based on strengthening hygiene and aseptic measures, promoting rational prescribing and combating self-medication.},
year = {2025}
}
TY - JOUR
T1 - Bacteriological Profile, Prevention and Control of Nosocomial Infections
AU - Salifou Traoré
AU - Ousmane Dembélé
AU - Madou Traore
AU - Kateneme Seydou Ouattara
AU - Oumar Berthé
AU - Siaka Coulibaly
AU - Aly Diallo
AU - Bathio Traoré
AU - Moussa Diassana
AU - Bernard Coulibaly
AU - Ahmadou Dembélé
AU - Abdou Dolo
AU - Moussa Kanté
AU - Soumaila Traoré
AU - Moussa Coulibaly
AU - Ternan Traoré
AU - Luka Diarra
AU - Hassan Souleymane
Y1 - 2025/02/10
PY - 2025
N1 - https://doi.org/10.11648/j.ajbls.20251301.15
DO - 10.11648/j.ajbls.20251301.15
T2 - American Journal of Biomedical and Life Sciences
JF - American Journal of Biomedical and Life Sciences
JO - American Journal of Biomedical and Life Sciences
SP - 31
EP - 35
PB - Science Publishing Group
SN - 2330-880X
UR - https://doi.org/10.11648/j.ajbls.20251301.15
AB - Our objective was to know the bacteriological profile of nosocomial infections and determine the risk factors in order to effectively fight against this scourge. Descriptive and retrospective study carried out in our department from April 30 to December 31, 2023, i.e. a period of 8 months. A total of 105 patients operated on for clean surgery were enrolled with a sex ratio of 9.5 ∕1 in favour of male sex. They came from the Sikasso region and the neighbouring countries (RCI and B Faso). Average age: 54.77±21.70 (3-85 years). Antibiotic prophylaxis based on ceftriaxone or Amoxy Clavulanic Acid instituted in all our patients. 15/105 developed a nosocomial infection, i.e. an incidence of 14.28%. The two types of infection are: Surgical site infection SSI, which is the predominant form with a rate of 73.30%, followed by infection associated with urethral catheterization, i.e. 26.66%. Cytobacteriological analysis of the samples made it possible to isolate germs in 13 patients, while they were sterile in the other two. These E Coli and K Pneumonia germs have been shown to be sensitive to imipenem, amikacin and fosfomycin. Length of stay, history of bladder catheterization and classic open surgery were proven risk factors. Nosocomial infection remains a real public health problem. Fighting against this scourge requires the establishment of regular monitoring system and good prevention policy based on strengthening hygiene and aseptic measures, promoting rational prescribing and combating self-medication.
VL - 13
IS - 1
ER -