Background: Imatinib, a name of assurance in the treatment of CML, not only brings significant prognosis and remission but also improves the quality of life of a patient. The study aimed to evaluate the efficacy of Imatinib in CML patients. Methods: This study was cross-sectional and multi-centered, starting from 2019-2024 from Sylhet, Chittagong, and Rajshahi. In this study, 529 patients were enrolled. Among them, 442 patients were taken, rest of the patients declined as BCR- ABL1 observed copies were <10,000. Sampling was done by convenient technique. Result: The patients' ages ranged from under 20 to over 80 years, with the majority falling between 21-30 years (25.71%) and 31-40 years (23.25%). The majority of the patients were male (57.66%). According to the analytical result, 442 patients (83.55%) tested positive. Among the 442 participants who tested positive for BCR-ABL1 mRNA, 155 patients (35.07%) were in remission. In contrast, 287 patients (64.93%) were not in remission, with an IS ratio greater than 0.1%. Among the 155 patients classified as in remission according to the IS ratio (≤0.1%), all 155 (100.00%) were also in remission according to the transcript percent ratio (≤10%). The sensitivity of the transcript percent ratio in identifying patients in remission was 100.00%, indicating that all patients in remission according to the IS categorization were also identified as in remission by the transcript percent ratio. The specificity was 36.60%, reflecting a lower ability to correctly identify patients not in remission. Conclusion: In the case of specificity, International-scale and large-scale clinical studies with long-term patient outcomes are more recommended.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
In chronic myeloid leukemia (CML), a clonal mylo-proliferative disorder of the hematopoietic stem, 95% cases are characterized by Philadelphia chromosome as the sole genetic abnormality into blast crisis. From previous studies, it is evident that, 1 to 2 cases per 100 000 per year are affected with CML annually
[1]
Druker BJ. Translation of the Philadelphia chromosome into therapy for CML. Blood, The Journal of the American Society of Hematology. 2008 Dec 15; 112(13): 4808-17.
[1]
. Without early diagnosis and proper treatment, the chronic phase (CP) of CML undergoes blast crisis (BC) whereas, the prognosis is poor
[2]
Wang L, Li L, Chen R, Huang X, Ye X. Understanding and monitoring chronic myeloid leukemia blast crisis: how to better manage patients. Cancer Management and Research. 2021 Jun 23: 4987-5000.
[2]
. The deleted chromosome 22 is produced by the reciprocal (but not fully balanced) translocation between the long arms of chromosomes 9 and 22. During this event, two genes, Abelson 1 (ABL1), located on chromosome 9, and the Breakpoint Cluster Region (BCR), on chromosome 22, generate a fusion gene called BCR-ABL1, that, along with the Philadelphia chromosome, which is the main diagnostic marker of CML
[3]
Chereda B, Melo JV. Natural course and biology of CML. Annals of hematology. 2015 Apr; 94: 107-21.
[3]
.
There are three phases of CML. 90% of patients are diagnosed in the chronic phase (CP), and the other two phases are the accelerated phase (AP) and the blast phase (BP)
[4]
Quintás-Cardama A, Cortes JE. Chronic myeloid leukemia: diagnosis and treatment. InMayo Clinic Proceedings 2006 Jul 1 (Vol. 81, No. 7, pp. 973-988). Elsevier.
[4]
. In previous studies, we have found that the average age of CML is around 64 years. Almost half of cases are diagnosed in people 65 and older. Children are rarely affected by this disease
[5]
Hijiya N, Suttorp M. How I treat chronic myeloid leukemia in children and adolescents. Blood, The Journal of the American Society of Hematology. 2019 May 30; 133(22): 2374-84.
[5]
.
Most of the CML patients do not have significant diagnostic symptoms. Some of common complaints from the patients are fatigue, weight loss, malaise and anemia. On laboratory findings, leukocytosis is a common finding, whereas platelet count can be high or low
[6]
Savage DG, Szydlo RM, Goldman JM. Clinical features at diagnosis in 430 patients with chronic myeloid leukaemia seen at a referral centre over a 16-year period. British journal of haematology. 1997 Jan; 96(1): 111-6.
[6]
. In 20-40 cases of CML, Splenomegaly is a common clinical manifestation. In case of prognosis of CML, it depends on the early diagnosis. The greatest diagnostic difficulty is patients having splenomegaly and leukocytosis but who do not have the Ph chromosome. Blood test and other laboratory tests are not able to clear the arising confusion. In these cases, the BCR-ABL1 hybrid gene can be recommended as a diagnostic tool. Patients achieving Ph negative and BCR-ABL1 negative are considered to be Ph-negative CML or chronic myelomonocytic leukemia
[7]
Jabbour E, Kantarjian H. Chronic myeloid leukemia: 2020 update on diagnosis, therapy and monitoring. American journal of hematology. 2020 Jun; 95(6): 691-709.
[7]
.
Imatinib, a pioneer drug of CML, recommended by FDA (Food Drug Administration) in the year of 2001, is recognized as the first signal transduction inhibitor (STI), to decline the oncologic pathway from BCR-ABL protein. It directly inhibits the constitutive tyrosine kinase activity. Once Imatinib is started, there is a significant decrease rate of mutation. The ultimate outcome of this drug is, modification of the function of various genes involved in the control of the cell cycle, cell adhesion, cytoskeleton organization and finally in the apoptotic death of Ph (+) cells. The oral bioavailability and terminal half-life are 98% and 18 hours respectively
[8]
Sacha T. Imatinib in chronic myeloid leukemia: an overview. Mediterr J Hematol Infect Dis. 2014 Jan 2; 6(1): e2014007.
[8]
. From the last 15 years of clinical studies, Imatinib and second-generation TKIs dramatically improved the prognosis of the disease
[9]
Mahon FX. Treatment-free remission in CML: who, how, and why?. Hematology 2014, the American Society of Hematology Education Program Book. 2017 Dec 8; 2017(1): 102-9.
[9]
.
In spite of having a high response of Imatinib in CML, there is a possibility of recurrence of CML if the drug is discontinued. Among the 3 phases of CML, Imatinib responds in CP, compared to the other phases. For a satisfactory prognosis of CML patients, 400 mg Imatinib is recommended
[10]
O'Hare T, Eide CA, Deininger MW. Bcr-Abl kinase domain mutations, drug resistance, and the road to a cure for chronic myeloid leukemia. Blood, The Journal of the American Society of Hematology. 2007 Oct 1; 110(7): 2242-9.
[10]
. By the BCR-ABL test, we can detect abnormal genes from the blood or bone marrow in CML patients. Real-time PCR has become the most acceptable method for monitoring BCR-ABL transcript levels of patients treated with kinase inhibitors
[11]
Machado MP, Tomaz JP, Lorand-Metze I, de Souza CA, Vigorito AC, Delamain MT, Bendit I, Pereira NF, Pagnano KB. Monitoring of BCR-ABL levels in chronic myeloid leukemia patients treated with imatinib in the chronic phase - the importance of a major molecular response. Rev Bras Hematol Hemoter. 2011; 33(3): 211-5.
[11]
. This study aimed to evaluate the efficacy of Imatinib in CML patients.
2. Methods
This study was cross-sectional and multi-centered, starting from 2019-2024 from Sylhet, Chittagong and Rajshahi. In this study, 529 patients were enrolled. Among them, 442 patients were taken, rest of the patients are declined as BCR- ABL1 observed copies were <10,000. Sampling was done by convenient technique.
Collecting all the information by using a data collection sheet that contained a structured Questionnaire along with baseline, demographic and clinical data. All information regarding clinical features were recorded in the information collection sheets with written consent from the respondents.
All the information were entered in SPSS for analysis (version 25.0; IBM Corp). We performed frequency analysis as an analytic study to observe the age, gender and the remission status of the respondents (Chi-square).
Inclusion Criteria:
1) Patients with CML.
2) Patient with written consent.
Exclusion Criteria:
1) Other malignancies.
2) Refuse to give consent.
3) Mentally unstable patients.
3. Result
Table 1. Distribution of the Respondents according to the Age.
Age Range (year)
Frequency
Percentage
≤20
59
11.15%
21-30
136
25.71%
31-40
123
23.25%
41-50
93
17.58%
51-60
91
17.20%
61-70
19
3.59%
71-80
6
1.13%
>80
2
0.38%
Mean±SD Age
37.92±14.63
Table 1 resembled distribution of the respondents according to the age. The patients' ages ranged from under 20 to over 80 years, with the majority falling between 21-30 years (25.71%) and 31-40 years (23.25%).
Table 2. Distribution of the Respondents according to the Gender.
Gender
Frequency
Percentage
Male
305
57.66%
Female
224
42.34%
Table 2 resembled distribution of the respondents according to the gender. Majority of the patients were male (57.66%).
Table 3. Distribution of the Respondents according to the analytical result.
Result
Frequency
Percentage
Negative
87
16.45%
Positive
442
83.55%
Table 3 shows distribution of the respondents according to the analytical result. It is evident that, 442 patients (83.55%) tested positive.
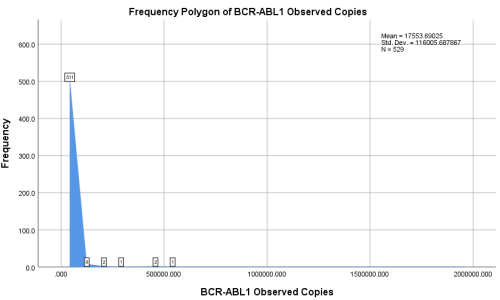
Figure 1 showed majority of patients had a lower number of observed copies, with a steep decline as the number of copies increased. The mean number of BCR-ABL1 observed copies was 17,553.69, with a standard deviation of 116,005.69, indicating a high variability among the patients.
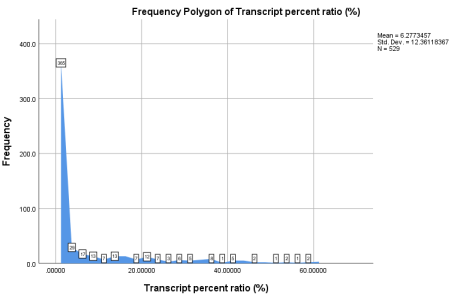
Figure 2. Frequency polygon of Transcript percent ratio.
Similar to the observed copies, the transcript percent ratio also showed a high frequency of lower values, with the majority of patients having a ratio close to zero. The mean transcript percent ratio was 6.28%, with a standard deviation of 12.36%, again indicating significant variability.
Table 3. Observation of patient remission status according to transcript percent ratio (n=442).
BCR-ABL1/ABL1 Transcript Percent Ratio
Frequency
Percentage
In remission (≤10%)
337
76.24%
No Remission (>10%)
105
23.76%
Mean±SD
7.51±13.18
Table 3 illustrated observation of patient remission status according to transcript percent ratio. Out of the 442 positive cases, 337 patients (76.24%) were in remission, defined as having a BCR-ABL1/ABL1 transcript percent ratio of ≤10%. Conversely, 105 patients (23.76%) were not in remission, with a transcript percent ratio greater than 10%. The mean transcript percent ratio for this group was 7.51%, with a standard deviation of 13.18%.
Table 4. Observation of patient remission status according to International Scale.
BCR-ABL1/ABL1 IS Ratio
Frequency
Percentage
In remission (≤0.1%)
155
35.07%
No Remission (>0.1%)
287
64.93%
Mean±SD
4.93±8.67
Table 4 showed observation of patient remission status according to international scale. Among the 442 participants who tested positive for BCR-ABL1 mRNA, 155 patients (35.07%) were in remission, defined as having a BCR-ABL1/ABL1 IS ratio of ≤0.1%. In contrast, 287 patients (64.93%) were not in remission, with an IS ratio greater than 0.1%. The mean IS ratio for this group was 4.93, with a standard deviation of 8.67.
Table 5 above showed correlation between IS and transcript percent ratio categorizations. Among the 155 patients classified as in remission according to the IS ratio (≤0.1%), all 155 (100.00%) were also in remission according to the transcript percent ratio (≤10%). In contrast, among the 287 patients classified as not in remission according to the IS ratio (>0.1%), 182 (63.41%) were in remission according to the transcript percent ratio, while 105 (36.59%) were not in remission according to the transcript percent ratio. The chi-square test revealed a significant correlation between the IS ratio and the transcript percent ratio (p-value <0.001).
Table 5. Correlation between IS and Transcript percent ratio categorizations.
Transcript Percent Ratio
International Scale
p-value (Chi-square test)
In Remission (n=155)
No Remission (n=287)
n
%
n
%
In Remission
155
100.00%
182
63.41%
<0.001
No Remission
0
0.00%
105
36.59%
Table 6. International Scale (IS) categorization as the gold standard.
Transcript Percent Ratio
International Scale
Total
In Remission
No Remission
In Remission
155 (TP)
182 (FP)
337
No Remission
0 (FN)
105 (TN)
105
Total
155
287
442
Table 6 showed Using the International Scale (IS) categorization as the gold standard, we evaluated the correlation between patient remission status as defined by the IS ratio and the transcript percent ratio. Among the 442 participants, 155 patients were correctly identified as in remission by both the transcript percent ratio and the IS categorization (True Positives, TP), while 182 patients were incorrectly identified as in remission by the transcript percent ratio but were not in remission according to the IS categorization (False Positives, FP). There were no patients incorrectly identified as not in remission by the transcript percent ratio but in remission according to the IS categorization (False Negatives, FN). Additionally, 105 patients were correctly identified as not in remission by both the transcript percent ratio and the IS categorization (True Negatives, TN). This analysis revealed a significant correlation between the IS ratio and the transcript percent ratio (p-value <0.001), indicating a strong association between the two measures. These findings highlight the specificity and sensitivity of the transcript percent ratio in identifying patient remission status when using the IS categorization as the gold standard.
Table 7. Sensitivity, Specificity, Accuracy, PPV, and NPV according to respondents.
Metric
Value
Simplified Formula
Sensitivity
100.00%
"TP / (TP + FN) * 100"
Specificity
36.60%
"TN / (TN + FP) * 100"
Accuracy
58.80%
"(TP + TN) / Total * 100"
Positive Predictive Value (PPV)
46.00%
"TP / (TP + FP) * 100"
Negative Predictive Value (NPV)
100.00%
"TN / (TN + FN) * 100"
Table 7 showed Sensitivity, Specificity, Accuracy, PPV, and NPV according to respondents. The sensitivity of the transcript percent ratio in identifying patients in remission was 100.00%, indicating that all patients in remission according to the IS categorization were also identified as in remission by the transcript percent ratio. The specificity was 36.60%, reflecting a lower ability to correctly identify patients not in remission. The accuracy of the transcript percent ratio was 58.80%, showing the overall correctness of the test. The positive predictive value (PPV) was 46.00%, indicating that less than half of the patients identified as in remission by the transcript percent ratio were correctly identified. The negative predictive value (NPV) was 100.00%, showing that all patients identified as not in remission by the transcript percent ratio were indeed not in remission according to the IS categorization.
4. Discussion
This cross-sectional multi-centered study, starting from 2019-2024 from Sylhet, Chittagong and Rajshahi. In this study, 529 patients were enrolled. Among them, 442 patients were taken, rest of the patients are declined as BCR- ABL1 observed copies were <10,000. Sampling was done by convenient technique.
In Ethopia, there was a study that occurred among 962 cases of CML diagnosis, the median age was 33 years and the majority presented with features of advanced-phase disease
[12]
Tadesse F, Asres G, Abubeker A, Gebremedhin A, Radich J. Spectrum of BCR-ABL Mutations and Treatment Outcomes in Ethiopian Imatinib-Resistant Patients With Chronic Myeloid Leukemia. JCO Glob Oncol. 2021 Jul; 7: 1187-1193.
[12]
. another similar study showed The mean age of respondents was 39.75 ±1.76 years
[13]
Bhamidipati PK, Kantarjian H, Cortes J, Cornelison AM, Jabbour E. Management of imatinib-resistant patients with chronic myeloid leukemia. Ther Adv Hematol. 2013 Apr; 4(2): 103-17.
[13]
. In our study, the majority of patients fell between 21-30 years (25.71%) and 31-40 years (23.25%).
In this study, Out of the 442 positive cases, 337 patients (76.24%) were in remission, defined as having a BCR-ABL1/ABL1 transcript percent ratio of ≤10%. All 155 (100.00%) were also in remission according to the transcript percent ratio (≤10%). In contrast, among the 287 patients classified as not in remission according to the IS ratio (>0.1%), 182 (63.41%) were in remission according to the transcript percent ratio, while 105 (36.59%) were not in remission according to the transcript percent ratio. The chi-square test revealed a significant correlation between the IS ratio and the transcript percent ratio (p-value <0.001). Similarly, there is an Iris trial whereas for 106 patients, the estimated PFS rates at 12 months and 36 months after the dose escalation were 94% and 89%, respectively. Complete molecular response (CMR) rates were 0% versus 43.8% respectively (p = 0.002), and no molecular responses were observed when adherence rates were 80% or lower. Lower adherence rates have been described in younger patients, those who experience adverse events (AEs) related to therapy, and those who require dose escalations
[14]
Hughes TP, Hochhaus A, Branford S, Müller MC, Kaeda JS, Foroni L, Druker BJ, Guilhot F, Larson RA, O'Brien SG, Rudoltz MS, Mone M, Wehrle E, Modur V, Goldman JM, Radich JP; IRIS investigators. Long-term prognostic significance of early molecular response to imatinib in newly diagnosed chronic myeloid leukemia: an analysis from the International Randomized Study of Interferon and STI571 (IRIS). Blood. 2010 Nov 11; 116(19): 3758-65.
[14]
. In the year of 2014, there was a similar study, where all outcomes were significantly superior for the 410 patients with BCR-ABL1 ≤10% which strongly indicated remission at 3 months (P <.001)
[15]
Branford S, Yeung DT, Parker WT, Roberts ND, Purins L, Braley JA, Altamura HK, Yeoman AL, Georgievski J, Jamison BA, Phillis S, Donaldson Z, Leong M, Fletcher L, Seymour JF, Grigg AP, Ross DM, Hughes TP. Prognosis for patients with CML and >10% BCR-ABL1 after 3 months of imatinib depends on the rate of BCR-ABL1 decline. Blood. 2014 Jul 24; 124(4): 511-8.
[15]
.
Imatinib, a magical hope in CML, not only helps in satisfactory remission but also improve the quality of life of patients, that may help people to lead a nearly normal lifespan. In previous cases, Undetectable BCR-ABL patients who have stopped treatment had a minimum chance of recurrence of the disease. There was only 10% chance of their disease coming back after the cessation of the treatment
[16]
Atallah E, Sweet K. Treatment-free remission: the new goal in CML therapy. Current Hematologic Malignancy Reports. 2021 Oct 1: 1-7.
[16]
. Overall, only efficacy and safety are not the concern in case of treatment, it is also mandatory to maintain the quality of life.
5. Limitation of the Study
105 patients were correctly identified as not in remission by both the transcript percent ratio and the IS categorization (True Negatives, TN). After 6 months of treatment, they might be in remission. Moreover, at the beginning of the study, only the Transcript percent ratio was available. So there may be some technological errors.
6. Conclusion
In this study, the transcript percentage ratio is not an ideal scale as the specificity percentage is low. However, limited data and lack of funding for treatment and lab equipment are some of the biggest obstacles to improving quality of life (HRQoL), especially in our country. More clinical trials and social awareness will be expected for better outcomes.
Abbreviations
BCR-ABL
Breakpoint Cluster Region-Abelson Proto-Oncogene
CML
Chronic Myeloid Leukemia
CP
Chronic Phase
SD
Standard Deviation
TKI
Tyrosine Kinase Inhibitor
Conflicts of Interest
The authors declare no conflicts of interest.
References
[1]
Druker BJ. Translation of the Philadelphia chromosome into therapy for CML. Blood, The Journal of the American Society of Hematology. 2008 Dec 15; 112(13): 4808-17.
[2]
Wang L, Li L, Chen R, Huang X, Ye X. Understanding and monitoring chronic myeloid leukemia blast crisis: how to better manage patients. Cancer Management and Research. 2021 Jun 23: 4987-5000.
[3]
Chereda B, Melo JV. Natural course and biology of CML. Annals of hematology. 2015 Apr; 94: 107-21.
[4]
Quintás-Cardama A, Cortes JE. Chronic myeloid leukemia: diagnosis and treatment. InMayo Clinic Proceedings 2006 Jul 1 (Vol. 81, No. 7, pp. 973-988). Elsevier.
[5]
Hijiya N, Suttorp M. How I treat chronic myeloid leukemia in children and adolescents. Blood, The Journal of the American Society of Hematology. 2019 May 30; 133(22): 2374-84.
[6]
Savage DG, Szydlo RM, Goldman JM. Clinical features at diagnosis in 430 patients with chronic myeloid leukaemia seen at a referral centre over a 16-year period. British journal of haematology. 1997 Jan; 96(1): 111-6.
[7]
Jabbour E, Kantarjian H. Chronic myeloid leukemia: 2020 update on diagnosis, therapy and monitoring. American journal of hematology. 2020 Jun; 95(6): 691-709.
[8]
Sacha T. Imatinib in chronic myeloid leukemia: an overview. Mediterr J Hematol Infect Dis. 2014 Jan 2; 6(1): e2014007.
[9]
Mahon FX. Treatment-free remission in CML: who, how, and why?. Hematology 2014, the American Society of Hematology Education Program Book. 2017 Dec 8; 2017(1): 102-9.
[10]
O'Hare T, Eide CA, Deininger MW. Bcr-Abl kinase domain mutations, drug resistance, and the road to a cure for chronic myeloid leukemia. Blood, The Journal of the American Society of Hematology. 2007 Oct 1; 110(7): 2242-9.
[11]
Machado MP, Tomaz JP, Lorand-Metze I, de Souza CA, Vigorito AC, Delamain MT, Bendit I, Pereira NF, Pagnano KB. Monitoring of BCR-ABL levels in chronic myeloid leukemia patients treated with imatinib in the chronic phase - the importance of a major molecular response. Rev Bras Hematol Hemoter. 2011; 33(3): 211-5.
[12]
Tadesse F, Asres G, Abubeker A, Gebremedhin A, Radich J. Spectrum of BCR-ABL Mutations and Treatment Outcomes in Ethiopian Imatinib-Resistant Patients With Chronic Myeloid Leukemia. JCO Glob Oncol. 2021 Jul; 7: 1187-1193.
[13]
Bhamidipati PK, Kantarjian H, Cortes J, Cornelison AM, Jabbour E. Management of imatinib-resistant patients with chronic myeloid leukemia. Ther Adv Hematol. 2013 Apr; 4(2): 103-17.
[14]
Hughes TP, Hochhaus A, Branford S, Müller MC, Kaeda JS, Foroni L, Druker BJ, Guilhot F, Larson RA, O'Brien SG, Rudoltz MS, Mone M, Wehrle E, Modur V, Goldman JM, Radich JP; IRIS investigators. Long-term prognostic significance of early molecular response to imatinib in newly diagnosed chronic myeloid leukemia: an analysis from the International Randomized Study of Interferon and STI571 (IRIS). Blood. 2010 Nov 11; 116(19): 3758-65.
[15]
Branford S, Yeung DT, Parker WT, Roberts ND, Purins L, Braley JA, Altamura HK, Yeoman AL, Georgievski J, Jamison BA, Phillis S, Donaldson Z, Leong M, Fletcher L, Seymour JF, Grigg AP, Ross DM, Hughes TP. Prognosis for patients with CML and >10% BCR-ABL1 after 3 months of imatinib depends on the rate of BCR-ABL1 decline. Blood. 2014 Jul 24; 124(4): 511-8.
[16]
Atallah E, Sweet K. Treatment-free remission: the new goal in CML therapy. Current Hematologic Malignancy Reports. 2021 Oct 1: 1-7.
Halder, S., Sinthia, K. A., Mahmud, T. (2025). Efficacy of Imatinib According to BCR-ABL Mutation in Patients with CML; Multi-Centered Analytical Study. American Journal of Biomedical and Life Sciences, 13(2), 47-52. https://doi.org/10.11648/j.ajbls.20251302.11
Halder, S.; Sinthia, K. A.; Mahmud, T. Efficacy of Imatinib According to BCR-ABL Mutation in Patients with CML; Multi-Centered Analytical Study. Am. J. Biomed. Life Sci.2025, 13(2), 47-52. doi: 10.11648/j.ajbls.20251302.11
Halder S, Sinthia KA, Mahmud T. Efficacy of Imatinib According to BCR-ABL Mutation in Patients with CML; Multi-Centered Analytical Study. Am J Biomed Life Sci. 2025;13(2):47-52. doi: 10.11648/j.ajbls.20251302.11
@article{10.11648/j.ajbls.20251302.11,
author = {Satyajit Halder and Khaleda Akter Sinthia and Tasnim Mahmud},
title = {Efficacy of Imatinib According to BCR-ABL Mutation in Patients with CML; Multi-Centered Analytical Study
},
journal = {American Journal of Biomedical and Life Sciences},
volume = {13},
number = {2},
pages = {47-52},
doi = {10.11648/j.ajbls.20251302.11},
url = {https://doi.org/10.11648/j.ajbls.20251302.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajbls.20251302.11},
abstract = {Background: Imatinib, a name of assurance in the treatment of CML, not only brings significant prognosis and remission but also improves the quality of life of a patient. The study aimed to evaluate the efficacy of Imatinib in CML patients. Methods: This study was cross-sectional and multi-centered, starting from 2019-2024 from Sylhet, Chittagong, and Rajshahi. In this study, 529 patients were enrolled. Among them, 442 patients were taken, rest of the patients declined as BCR- ABL1 observed copies were Result: The patients' ages ranged from under 20 to over 80 years, with the majority falling between 21-30 years (25.71%) and 31-40 years (23.25%). The majority of the patients were male (57.66%). According to the analytical result, 442 patients (83.55%) tested positive. Among the 442 participants who tested positive for BCR-ABL1 mRNA, 155 patients (35.07%) were in remission. In contrast, 287 patients (64.93%) were not in remission, with an IS ratio greater than 0.1%. Among the 155 patients classified as in remission according to the IS ratio (≤0.1%), all 155 (100.00%) were also in remission according to the transcript percent ratio (≤10%). The sensitivity of the transcript percent ratio in identifying patients in remission was 100.00%, indicating that all patients in remission according to the IS categorization were also identified as in remission by the transcript percent ratio. The specificity was 36.60%, reflecting a lower ability to correctly identify patients not in remission. Conclusion: In the case of specificity, International-scale and large-scale clinical studies with long-term patient outcomes are more recommended.
},
year = {2025}
}
TY - JOUR
T1 - Efficacy of Imatinib According to BCR-ABL Mutation in Patients with CML; Multi-Centered Analytical Study
AU - Satyajit Halder
AU - Khaleda Akter Sinthia
AU - Tasnim Mahmud
Y1 - 2025/03/06
PY - 2025
N1 - https://doi.org/10.11648/j.ajbls.20251302.11
DO - 10.11648/j.ajbls.20251302.11
T2 - American Journal of Biomedical and Life Sciences
JF - American Journal of Biomedical and Life Sciences
JO - American Journal of Biomedical and Life Sciences
SP - 47
EP - 52
PB - Science Publishing Group
SN - 2330-880X
UR - https://doi.org/10.11648/j.ajbls.20251302.11
AB - Background: Imatinib, a name of assurance in the treatment of CML, not only brings significant prognosis and remission but also improves the quality of life of a patient. The study aimed to evaluate the efficacy of Imatinib in CML patients. Methods: This study was cross-sectional and multi-centered, starting from 2019-2024 from Sylhet, Chittagong, and Rajshahi. In this study, 529 patients were enrolled. Among them, 442 patients were taken, rest of the patients declined as BCR- ABL1 observed copies were Result: The patients' ages ranged from under 20 to over 80 years, with the majority falling between 21-30 years (25.71%) and 31-40 years (23.25%). The majority of the patients were male (57.66%). According to the analytical result, 442 patients (83.55%) tested positive. Among the 442 participants who tested positive for BCR-ABL1 mRNA, 155 patients (35.07%) were in remission. In contrast, 287 patients (64.93%) were not in remission, with an IS ratio greater than 0.1%. Among the 155 patients classified as in remission according to the IS ratio (≤0.1%), all 155 (100.00%) were also in remission according to the transcript percent ratio (≤10%). The sensitivity of the transcript percent ratio in identifying patients in remission was 100.00%, indicating that all patients in remission according to the IS categorization were also identified as in remission by the transcript percent ratio. The specificity was 36.60%, reflecting a lower ability to correctly identify patients not in remission. Conclusion: In the case of specificity, International-scale and large-scale clinical studies with long-term patient outcomes are more recommended.
VL - 13
IS - 2
ER -
Halder, S., Sinthia, K. A., Mahmud, T. (2025). Efficacy of Imatinib According to BCR-ABL Mutation in Patients with CML; Multi-Centered Analytical Study. American Journal of Biomedical and Life Sciences, 13(2), 47-52. https://doi.org/10.11648/j.ajbls.20251302.11
Halder, S.; Sinthia, K. A.; Mahmud, T. Efficacy of Imatinib According to BCR-ABL Mutation in Patients with CML; Multi-Centered Analytical Study. Am. J. Biomed. Life Sci.2025, 13(2), 47-52. doi: 10.11648/j.ajbls.20251302.11
Halder S, Sinthia KA, Mahmud T. Efficacy of Imatinib According to BCR-ABL Mutation in Patients with CML; Multi-Centered Analytical Study. Am J Biomed Life Sci. 2025;13(2):47-52. doi: 10.11648/j.ajbls.20251302.11
@article{10.11648/j.ajbls.20251302.11,
author = {Satyajit Halder and Khaleda Akter Sinthia and Tasnim Mahmud},
title = {Efficacy of Imatinib According to BCR-ABL Mutation in Patients with CML; Multi-Centered Analytical Study
},
journal = {American Journal of Biomedical and Life Sciences},
volume = {13},
number = {2},
pages = {47-52},
doi = {10.11648/j.ajbls.20251302.11},
url = {https://doi.org/10.11648/j.ajbls.20251302.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajbls.20251302.11},
abstract = {Background: Imatinib, a name of assurance in the treatment of CML, not only brings significant prognosis and remission but also improves the quality of life of a patient. The study aimed to evaluate the efficacy of Imatinib in CML patients. Methods: This study was cross-sectional and multi-centered, starting from 2019-2024 from Sylhet, Chittagong, and Rajshahi. In this study, 529 patients were enrolled. Among them, 442 patients were taken, rest of the patients declined as BCR- ABL1 observed copies were Result: The patients' ages ranged from under 20 to over 80 years, with the majority falling between 21-30 years (25.71%) and 31-40 years (23.25%). The majority of the patients were male (57.66%). According to the analytical result, 442 patients (83.55%) tested positive. Among the 442 participants who tested positive for BCR-ABL1 mRNA, 155 patients (35.07%) were in remission. In contrast, 287 patients (64.93%) were not in remission, with an IS ratio greater than 0.1%. Among the 155 patients classified as in remission according to the IS ratio (≤0.1%), all 155 (100.00%) were also in remission according to the transcript percent ratio (≤10%). The sensitivity of the transcript percent ratio in identifying patients in remission was 100.00%, indicating that all patients in remission according to the IS categorization were also identified as in remission by the transcript percent ratio. The specificity was 36.60%, reflecting a lower ability to correctly identify patients not in remission. Conclusion: In the case of specificity, International-scale and large-scale clinical studies with long-term patient outcomes are more recommended.
},
year = {2025}
}
TY - JOUR
T1 - Efficacy of Imatinib According to BCR-ABL Mutation in Patients with CML; Multi-Centered Analytical Study
AU - Satyajit Halder
AU - Khaleda Akter Sinthia
AU - Tasnim Mahmud
Y1 - 2025/03/06
PY - 2025
N1 - https://doi.org/10.11648/j.ajbls.20251302.11
DO - 10.11648/j.ajbls.20251302.11
T2 - American Journal of Biomedical and Life Sciences
JF - American Journal of Biomedical and Life Sciences
JO - American Journal of Biomedical and Life Sciences
SP - 47
EP - 52
PB - Science Publishing Group
SN - 2330-880X
UR - https://doi.org/10.11648/j.ajbls.20251302.11
AB - Background: Imatinib, a name of assurance in the treatment of CML, not only brings significant prognosis and remission but also improves the quality of life of a patient. The study aimed to evaluate the efficacy of Imatinib in CML patients. Methods: This study was cross-sectional and multi-centered, starting from 2019-2024 from Sylhet, Chittagong, and Rajshahi. In this study, 529 patients were enrolled. Among them, 442 patients were taken, rest of the patients declined as BCR- ABL1 observed copies were Result: The patients' ages ranged from under 20 to over 80 years, with the majority falling between 21-30 years (25.71%) and 31-40 years (23.25%). The majority of the patients were male (57.66%). According to the analytical result, 442 patients (83.55%) tested positive. Among the 442 participants who tested positive for BCR-ABL1 mRNA, 155 patients (35.07%) were in remission. In contrast, 287 patients (64.93%) were not in remission, with an IS ratio greater than 0.1%. Among the 155 patients classified as in remission according to the IS ratio (≤0.1%), all 155 (100.00%) were also in remission according to the transcript percent ratio (≤10%). The sensitivity of the transcript percent ratio in identifying patients in remission was 100.00%, indicating that all patients in remission according to the IS categorization were also identified as in remission by the transcript percent ratio. The specificity was 36.60%, reflecting a lower ability to correctly identify patients not in remission. Conclusion: In the case of specificity, International-scale and large-scale clinical studies with long-term patient outcomes are more recommended.
VL - 13
IS - 2
ER -